It will end crappily though, I thought.
The typical patient with Parkinson’s becomes disabled after eight to 10 years, but this typical patient does not exist. Everyone is different. Six
years after being diagnosed, I was still on the tennis court. Then everything went wrong. Within a few months I became a wavering wreck. Walking turned into stumbling and I was forced to shuffle along behind a frame.
The time had come for brain surgery,
my neurologist declared, and I was admitted to a clinic in the north of the Netherlands “for
observation”. It took me several days to get used to the other patients. There were seven of them: three men and four women. I watched their nonsensical tremors and how they moved, step by petty step, as they tried desperately to swerve the wheels of
their walking frames in the right direction. They ate in silence. One of them, a grumpy farmer from the countryside, sat quietly urinating on the worn-out lift chair.
One patient, a man in his 70s with a sturdy head and a weathered gaze, sat opposite
me during dinner. Crouched like a frightened bird, he ate his sauerkraut mash while keeping his mouth close to the plate and drooling. From time to time some of the food fell back from his fork or from his raw, red swollen lower lip. When his plate was half
empty, a nurse mercifully fed him a few more bites. His chin sagged on to the plate, his gray beard dipping in the cold sauerkraut mash.
My God. I had pictured hallucinations. I
had read that Parkinson’s patients have a much greater risk of dementia. I had accepted that one day my wife would have to cut up my food and tie my shoelaces. I had scoured eBay for a reasonably-priced mobility scooter. I had more or less come to terms
with all that, but after spending time at the clinic, my neurologist’s remark – “It won’t kill you” – took on an entirely new meaning. If everything goes wrong, I thought, this is what lies ahead of me. And it won’t
even kill me.
What was worse? The looming oblivion of dementia or the cruel physical failures that come with Parkinson’s disease? Was it better to be trapped in a confused mind, or have a lucid mind while being trapped in a rebellious
body?
Over recent years, I had discussed these kinds of questions with a friend of mine named Joop. We met occasionally and talked about dying, as if we were discussing a long-term weather forecast. Joop suffered from Alzheimer’s and had started
to forget the basics of daily life. What he did know was that he didn’t want to die the way his father did, in a nursing home. “I don’t want to end up chasing after the nurses,” he told me.
Even as we replace old hips or knees
or organs with new ones, and even as average life expectancy continues to increase, our brains keep on ageing. Neurodegeneration is the price we pay for the intense human drive to deny that existence is finite. Sooner or later our brains start to falter, nerve
cells break down, and we end up in a nursing home, chasing nurses, chasing shadows, chasing ourselves.
I understood Joop’s deepest fear
only too well. Nico, my father-in-law, was 91 when, in the middle of the night, he mistook his wife for an intruder and attacked her with a kitchen knife. Shortly after the incident, he was placed in the closed ward of a geriatric facility. That image never
left my mind: the helplessness of the confused man we left behind when the lock of the glass door clicked, his bewildered eyes staring at us in an unstoppable kind of loneliness. Weeks later, when we were visiting Nico, he reproached his wife for neglecting
him. She never came to visit him, he grumbled, even though less than an hour beforehand she had fed him pieces of bread, with tears in her eyes.
On our way home, it hit me that I would rather die than end up like that. For the first time, I
seriously considered the possibility of one day voluntarily ending my life. After all, I thought, the Netherlands has the best-regulated voluntary euthanasia system in the world.
Until
the 1950s, the historian James Kennedy has argued, the Netherlands was more conservative, more religious and less prosperous than most other European countries. Then everything changed, and this fearful nation turned into a pioneer. We became an open, liberal
society that led the way on ethical issues. We tolerated drugs, legalised abortion, and our prostitutes paid taxes.
Where we had once been devout and Calvinist, in the 60s we entered a godforsaken era. Churches were turned into shops or apartments.
By the end of the century, Christian political parties had lost their grip on power, and their dogmas no longer dictated matters of life and death. The nation had long debated the question of whether assisted death should, in certain cases, be legalised. And
in 2001, the Dutch parliament voted to make the Netherlands the first nation in the world to legalise
euthanasia. Central to the argument in favour of the new law was the right to self-determination. “My death is my own,” as the Dutch say.
Today, nine out of 10 Dutch citizens support the euthanasia law, which went into effect in April 2002. This law allows physicians to honour requests to assist a patient who wants to end
their life, if there is “unbearable and hopeless suffering” with no hope of improvement. This means that a physician could, for example, prevent someone with lung cancer from dying choking in their own blood.
The debate did not cease once
the law was passed. New groups of patients demanded an even more liberal interpretation of the same law. And after every verdict that broadened the criteria for euthanasia, another group of citizens campaigned for even more progressive legislation. With every
new demand, the debate would fire up once again. Supporters see the expansion of the law as moral progress, while opponents predict that we are moving towards a society reminiscent of Nazi Germany, where we get rid of those deemed “useless”, such
as the very elderly or those with severe mental illness.
Nevertheless, the euthanasia debate seems to have entered a faltering phase. A very un-Dutch thing has happened.
We appear to be tongue-tied. The Netherlands – the country that, more than any other, wants to believe in every person’s right to voluntary death, the country that talks lightly about painless death as it were a money-back guarantee – is
struggling with the dilemma surrounding dementia and death.
Ifirst met Joop on a cold and rainy September day in 2012. He was in his 70s. A year after he was diagnosed
with Alzheimer’s, Joop was still remarkably fit. But when he started telling me the story of his choir and their performances in nursing homes for the third time in 20 minutes, I realised dementia had already disrupted his short-term memory.
Even
though Joop was unaware, in that moment at least, of how much his illness had already begun to eat away at his mind, he knew what was in store for him. He could not let go of the images he had seen in those nursing homes. He had decided that when the day eventually
came that he could no longer live with Janny, the love of his life, he would rather die.
“How do you think that day will go?” I asked him. He imagined that it would almost be an ordinary day. His children and grandchildren would come to
say goodbye. “And then the doctor will walk in and give me an injection,” he said.
That might have been somewhat naive. For some time, Janny and Joop had been looking for a doctor who would be willing to help him die at the time he had chosen:
the day when Joop was no longer capable of living at home. The doctors they had spoken to had explained that until Joop’s suffering was unbearable, they could not perform euthanasia. But when Joop asked, “What will you do when my dementia is more
severe and I’m incompetent?” the doctors explained that, at that stage, they could not perform euthanasia.
I don’t think Joop ever completely understood this catch-22. Dementia poses special problems for euthanasia cases. Under Dutch
law, a doctor is allowed to help a person with severe dementia to die, if that patient had prepared an advance euthanasia directive back when they were still mentally competent. Joop had one of those. He assumed everything had been arranged. But it hadn’t.
Of the 10,000 Dutch patients with dementia who die each year, roughly half of them will have had an advance euthanasia directive. They believed a doctor would “help” them. After all, this was permitted by law, and it was their express wish.
Their naive confidence is shared by four out of 10 Dutch adults, who are convinced that a doctor is bound by an advance directive. In fact, doctors are not obliged to do anything. Euthanasia may be legal, but it is not a right.
As doctors have a monopoly on merciful killing, their ethical standard, and not the law, ultimately determines whether a man like Joop can die. An advance directive is just one
factor, among many, that a doctor will consider when deciding on a euthanasia case. And even though the law says it’s legal, almost no doctors are willing to perform euthanasia on patients with severe dementia, since such patients
are no longer mentally capable of making a “well-considered request” to die.
This is the catch-22. If your dementia is at such an early stage that you are mentally fit enough to decide that you want to die, then it is probably “too
early” to want to die. You still have good years left. And yet, by the time your dementia has deteriorated to the point at which you wished (when your mind was intact) to die, you will no longer be allowed to die, as you are not mentally fit to make
that decision. It is now “too late” to die.
It is a sad story. The right to die has been discussed for so long now in the Netherlands that we have come to believe we each have the right to die when we want. But when push comes to shove,
the patient is not the one who decides on their euthanasia. It is the doctor who decides, and no one else. For the thousands of dementia patients who thought they would escape the worst of the disease, the Dutch euthanasia law is an utter failure. In
2017, there were 6,585 official cases of euthanasia in the Netherlands, the majority of them for cancer patients. By contrast, since 2012, only seven people with severe dementia died by euthanasia. Almost no one with dementia is able to die “on time”
– that is, when they actually wanted to.
In 2008, when he was no longer able to write, the Flemish author Hugo Claus, who had several times been tipped to win the Nobel prize for literature, chose euthanasia. Claus was suffering from Alzheimer’s,
but was mentally fit enough to make the decision to die. His decision was seen by many as “brave” but it was also strongly criticised, especially in Belgium, which had followed the Netherlands in legalising euthanasia but was still facing highly
outspoken Catholic opposition that considered euthanasia a grave sin.
And yet the death of Claus helped bring about a shift. According to the sociologist Hugo van der Wedden, those with dementia were given a voice, and were listened to more often than
before. The law itself didn’t change, but some doctors changed their interpretation of what constitutes unbearable suffering. The fear of future suffering was recognised by doctors as unbearable suffering itself and, as a result, some doctors are now
more willing to provide euthanasia to people in the early stages of dementia.
Still, the catch-22 remains. The patient must still be deemed mentally fit to confirm that they want to die. If they linger too long, if they want to see one more spring with
flowering apple trees, and subsequently slip into a deeper dementia, the opportunity for an early death will have passed. The only thing left will the long detour to the grave.
Since 2002, roughly 150,000 Dutch people with dementia have died. Tens of thousands of them stated their wish in an advance euthanasia directive. Yet most of them died “too late”, because choosing to die “too early”
proved to be too hard. During the first few years after the euthanasia law took effect, not a single patient with severe dementia died the dignified death that they had hoped for. In recent years, only one in a hundred patients with dementia managed to die
in the second-best way, which is “too early”. That was what happened to Joop, whose doctor helped him die on 8 May last year.
On a Monday evening in February
2016, 1.5 million Dutch viewers watched a woman named Hannie Goudriaan die on television.
In the documentary, we see Hannie just before her euthanasia. At one point, someone asks her whether she truly realises what is about to happen.
“What do you mean?” she answers.
Does she know why the doctor is stopping by?
“Oh,
I don’t know,” she says.
“You want to go, right?” asks her husband, Gerrit.
“I want, uhm, ready, well, just chop-chop.”
“Are you sure?” her husband asks.
“Yes.”
On
screen, Hannie Goudriaan is a woman of advanced age with thin, short gray hair, a surprised look and thin, tightly closed lips.
“Don’t you feel sorry for me?” her husband asks as the euthanasia doctor sits down opposite his wife.
“Yes,” Hannie says. “That’s why, chop-chop.”
“It’s time, baby,” Gerrit says. “Be brave now. You have been so very brave for so long.”
He puts his arms around her, his head on her
shoulder – as if he is looking for her to comfort him. Hannie lets it happen. Her husband holds her. From the drip needle attached to her left hand, a transparent tube is connected to the syringe that the doctor is holding. With his other hand he is
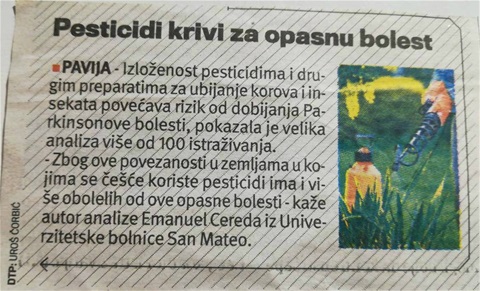
holding two fingers of Hannie’s left hand. Then the doctor injects the fluid into the vein. “It’s horrible,” Hannie, 68, says, before she dies.
Hannie Goudriaan (right) in a documentary about euthanasia shown on Dutch
TV in 2016. Photograph: NTR
Hannie Goudriaan had known where things were headed. She had semantic dementia, a rare disease that slowly and inescapably takes a person’s language away. Years earlier she had written a will, which stated that she wanted
to die as soon as she was no longer able to communicate properly. Her personal doctor considered her wish for a while, but felt he could not be certain that she wanted to die. He referred her to the End of Life clinic, established in 2012 by the NVVE, the Dutch Right to Die organisation. The clinic is where people can turn to when their doctor refuses to help them. However, the clinic does not guarantee
that it will be able to grant a death wish. Its physicians will consider the same question, which is: can this be done within the law?
The doctor who
helped Hannie to die, in 2015, a year before the documentary was broadcast, is Remco Verwer. He read her will and spoke to her case manager before conducting seven conversations with her. “There is nothing left, it is empty inside, I can no longer do
anything, I have lost everything, I want to go,” she said in a lucid moment. Verwer said: “She had become what she had never wanted to be.” After her death, the commission overseeing the practice of euthanasia determined that Verwer had handled
the case “with caution”.
And yet many viewers were stunned by what they saw on TV. “This is murder with one-and-a-half million witnesses,” Victor Lamme, a professor in cognitive neuroscience,
tweeted after having watched the documentary. A day later he repeated the raw accusation on De Wereld Draait Door, one of the most-watched primetime shows on Dutch television, while Verwer sat across from him and tried to explain that Lamme
had only seen what he wanted to see.
One reason the public was shocked is that they had actually seen how a doctor had ended a woman’s life. It’s one thing to vent your opinion on a euthanasia law that remains vague or
theoretical to you. Death entering your living room while you’re sipping your coffee is a different experience.
The documentary, which had aimed to show the reality of the End of Life Clinic, also revealed another truth. We are comfortable talking
about our own deaths, but when it comes to the deaths of other people, we feel differently. As much as we don’t want to end up in a nursing home, lost and lonely, a mere shadow of the people we once were, we will maintain that grandfather “seems
happy enough”, wandering through the hallways in his underwear.
Likewise, we value control over the end of our own lives, but cramp up when a loved one says she is “finished” with hers. “Isn’t it too soon?” we ask.
When we’re the ones staying behind, death seems harder to accept. Apparently, the death of a loved one is far more frightening to us than our own mortality. As the German sociologist Norbert Elias once said: “Death is a problem for the living.”
One Sunday last year, I ask my wife to join me in the garden, underneath the old apple tree. Finally, we discuss what lies ahead of us. “Growing old together shouldn’t
have been like this,” I say. “I am only half the man I used to be. I know. But you having to tie my shoelaces, push my wheelchair and maybe even feed me bites of sauerkraut mash … ”
“Don’t be silly,” my wife
says. “I have always known that this could happen. Or the other way around. That you would have to push me.”
That’s when I show her the envelope holding my advance euthanasia directive. It’s not an easy thing. What once seemed
a philosophical and political problem becomes absurdly different when you have to explain it to the one you’re leaving behind.
“I have
always known how you felt about this,” she says.
“I myself didn’t know for a long time.”
“Tell me,” she says.
“Daily inconveniences,” I say, “I am willing to bear. There is
simply no getting away from that. The stupid suffering. I will slowly become disabled – but I think I can live with that. Perhaps I will get used to the jerking of my head, the pain at night, the leg that always wants to go in another direction, and
the endless tapping of my fingers … maybe a nurse will have to give me sponge baths … good lord … as long as I’m able to read, I’m even willing to wear a diaper.”
I can see her thinking: you’re trying to
play it cool. Have I already forgotten what that nursing home was like?
“I couldn’t care less about dignity and decorum – those were gone the moment I wet myself for the first time. But if I no longer know where I am, if I begin to
disappear and become someone else, if I no longer recognise our children, then it’s time to close the book.”
The wind rises. The sweet smell of summer. She asks what it is that I want.
“I thought I knew. I thought I wanted to
stay a step ahead, to die in the early stage of dementia. I just had to find the courage to ask.”
“But … ?”
“Then I changed my mind. This is not about my courage.”
She stares at me,
sceptical, hesitant.
I try to explain that I’ve come to realise that my death is not a big deal to me. What do we know about death? Death is nothing. We will never have a clue about it. How could I possibly be afraid of it? There is no reason
to be. Why are we so obsessed with the idea that we must stay in control? For whom?
“This isn’t about me,” I say. I take a deep breath. “My death is not my own. My death will only ever mean something to those I leave behind.
And if I’m not terribly wrong, I won’t even know the half-death that severe dementia is supposed to be. Just let me go under, slowly drift off, past the point of nothingness, the point of no return.”
“There is not one doctor
that will help you,” she says.
“No. A doctor will not do that.”
I tell my love that I’ve made up my mind. “I hope it never happens, but if the day should come that I lose my mind and the ability to convince the doctor
of my wish to die, someone else will have to make the decision for me.”
“But doctors don’t do that.”
“No,
they don’t.”
“Then who?”
“The others. The ones who are left behind … ”
And then I explain to her, carefully searching for the right words, that I still believe in the right of self-determination.
We didn’t ask to grow old, did we? But in our desire to maintain self-control – a tragic and lonely desire – we sometimes forget about the others. I understand now that no one dies alone, that there are always those left behind who have to
deal with that. And that gives us the moral obligation to live on.
“The right to die,” I say, “must be the right to allow another person – not a doctor, but a loved one – to make the decision about the ending of your life.
That is a very big deal. If only because it is forbidden by law. That law must be changed, and that will take many years.”
She finds
it an impossible thought. How could anyone ask such a thing?
“You can say no.”
“And then what?”
“Then I’ll have to look for someone else. That is my only wish, that I am the one who decides who is to
make the decision.”
That thought is just as painful and impossible as the one before.
I try to calm her down. “It will be your decision when I die, whatever that may be.”
“Well, if that’s your choice …
” she says. Blossoms drift softly on to her lap.
She will help me, she says. As she has always done. “No matter what,” she says. “I will take care of you until your last breath.”
Translated by Nephtalie Demei
• Follow the Long Read on Twitter at @gdnlongread, or sign
up to the long read weekly email here.
https://www.theguardian.com/news/2018/aug/10/my-death-is-not-my-own-the-limits-of-legal-euthanasia